

ABSTRACT
Background and Aim: Feline polycystic kidney disease (PKD) is the most common inherited renal disorder in cats and is primarily associated with a nonsense mutation in the
Materials and Methods: This retrospective, single-center observational study included 28 client-owned cats evaluated by renal ultrasonography and
Results: All cats were clinically stable and non-azotemic at the time of evaluation. Conventional renal biomarkers did not differ significantly among groups. However, cats with renal cysts showed stronger associations between inflammatory indices and renal morphometric parameters compared with healthy controls. These correlations were most pronounced in cats harboring a heterozygous
Conclusion: Systemic inflammatory activation is detectable in cats with PKD before the onset of azotemia, particularly in those carrying
Keywords: biomarkers, feline polycystic kidney disease, inflammation, neutrophil-to-lymphocyte ratio, pkd1 mutation, renal morphometrics, Scottish Fold cats, ultrasonography.
INTRODUCTION
Cats have become increasingly popular companion animals, and advances in feline medicine have consequently placed greater emphasis on inherited disorders [1]. Polycystic kidney disease (PKD) is among the most common inherited renal disorders in cats and is characterized by the progressive development of multiple renal cysts in the absence of other underlying causes, such as elevated symmetric dimethylarginine (SDMA) [2–4]. Feline PKD is most frequently reported in Persian and Persian-related breeds and is inherited as an autosomal dominant trait [5]. The identification of causative genetic variants has substantially improved the understanding of PKD in cats. In particular, a nonsense mutation in the
Biomarkers are increasingly incorporated into veterinary practice for diagnostic and prognostic purposes because they provide rapid, objective, and reproducible information [10]. Our previous study identified peptides and proteins associated with familial PKD in cats using matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry combined with peptide mass fingerprinting and three-dimensional principal component analysis [11]. In addition, recent studies have demonstrated that kidney function screening can detect early renal deterioration at stages when the glomerular filtration rate has begun to decline [12]. Nevertheless, data on inflammation-related biomarkers in feline PKD remain limited, and their clinical relevance has not been fully elucidated [13].
Although PKD has been extensively characterized using ultrasonography and
The present study aimed to investigate the association between systemic inflammatory indices derived from routine hematological profiles and renal morphometric, biochemical, and genetic parameters in cats with PKD. Specifically, this study sought to evaluate whether inflammatory biomarkers are associated with renal cystic changes and
MATERIALS AND METHODS
Ethical approval
This study was conducted in accordance with institutional guidelines for the use of animals in research and was reviewed and approved by the Ethics Committee of Kasetsart University, Thailand, under approval number ACKU-65-VET-077. The study involved client-owned cats presented to the Kasetsart University Veterinary Teaching Hospital, Kamphaeng Saen, and was based on retrospective evaluation of medical records, renal ultrasonographic findings, hematological and biochemical data, and
Study period and location
This retrospective, single-center observational study was conducted at the Animal Teaching Hospital, Kamphaeng Saen, Faculty of Veterinary Medicine, Kasetsart University, Thailand. Medical records and biological samples were reviewed from cats presented between January 2024 and September 2025. The hospital functions as a referral center for companion animals in central Thailand, providing routine preventive care, diagnostic imaging, and advanced clinical services. The study workflow comprised case identification and eligibility screening, clinical and ultrasonographic assessment, laboratory and molecular analyses, and statistical evaluation.
Animals and selection of cases
A total of 28 client-owned cats (mean age 5.34 ± 2.25 years, body weight 3.50 ± 0.85 kg) were enrolled through convenience sampling based on the availability of complete clinical records and biological samples. Written informed consent was obtained from all owners before inclusion. Cats aged ≥1 year were eligible for enrollment. Exclusion criteria included concurrent chronic systemic diseases known to influence inflammatory or renal biomarkers, such as chronic kidney disease, diabetes mellitus, epilepsy, or other severe systemic illnesses, as determined by medical history, physical examination, and laboratory findings. All cats underwent standardized clinical evaluation, including assessment of sex, breed, age, body weight, and medical history. Routine diagnostic procedures included abdominal ultrasonography and blood profile analysis. Approximately 1 mL of blood was collected aseptically from peripheral veins and processed immediately for complete blood count (CBC) and serum biochemistry using standard hospital protocols.
Ultrasonographic examination
Renal ultrasonography was performed by an experienced veterinary clinician using a cardiac-capable ultrasound system equipped with a high-frequency transducer. Cats were examined in right- and left-lateral recumbency following routine abdominal imaging protocols. Still images and cine loops were digitally archived for subsequent analysis. Renal cysts were defined as well-circumscribed, anechoic structures with distal acoustic enhancement. Cats presenting with more than two renal cysts were classified as having PKD according to previously published criteria [14]. All measurements were obtained from recorded images, as illustrated in Figure 1.
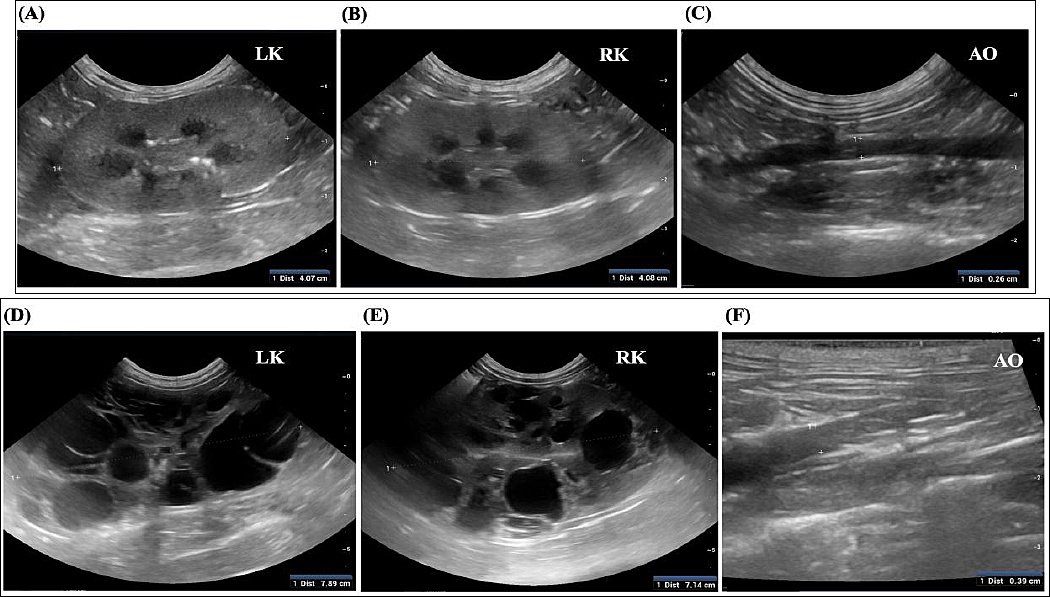
Figure 1. Ultrasonographic assessment of the left kidney (LK), right kidney (RK), and abdominal aorta (AO). (A–C) Control cat (Group 1). (D–F) Cat with a heterozygous
DNA extraction and polymerase chain reaction
Genomic DNA was extracted from frozen whole-blood samples using a commercial DNA extraction kit according to the manufacturer’s instructions. Detection of the
DNA sequencing
PCR products were purified using a commercial PCR purification kit before sequencing. Purified amplicons were subjected to Sanger sequencing using the same primer pairs as those used for PCR. Sequence chromatograms were analyzed and aligned using BioEdit software, and polymorphisms were identified by comparison with reference
Serum biomarker analysis
Serum samples were centrifuged and stored under appropriate conditions until analysis. Hematological data obtained from the CBC were used to calculate inflammatory indices, including neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), and PLR, following established veterinary methods. Serum C-reactive protein (CRP) concentrations were measured using a validated assay according to the manufacturer’s protocol. These biomarkers were selected to assess subclinical inflammatory status in cats with PKD.
Statistical analysis
Data were assessed for normality before analysis and are presented as mean ± SEM. Continuous variables were compared using Student’s t-test or one-way analysis of variance, as appropriate. Pearson’s correlation analysis was used to evaluate associations among renal imaging parameters, genetic status, and inflammatory biomarkers. A p-value < 0.05 was considered statistically significant. Statistical analyses were performed using GraphPad Prism software (version 10.0) in accordance with standard biostatistical guidelines.
RESULTS
Clinical characteristics and baseline findings
All cats included in the study were clinically stable at the time of evaluation. None exhibited overt clinical signs commonly associated with advanced renal disease, including anorexia, weight loss, vomiting, polyuria, polydipsia, lethargy, or dehydration. Physical examination parameters, including body condition score, hydration status, heart rate, respiratory rate, and blood pressure, were within acceptable age- and breed-specific reference ranges. Importantly, no cats were classified as azotemic, and none fulfilled the diagnostic criteria for chronic kidney disease at enrollment. No mortality events occurred during the study period, and no cats required euthanasia or were lost to follow-up because of renal-related complications. As this was a retrospective, clinically oriented study involving client-owned animals, postmortem examination and histopathological evaluation were not available and were therefore not included in the analysis.
Baseline characteristics of the study animals
The most prevalent breeds among the enrolled cats were Scottish Fold (n = 9, 32.14%), Persian (n = 7, 25%), domestic shorthair (n = 4, 14.28%), and mixed breeds (n = 8, 28.58%). Based on renal ultrasonographic findings and
Table 1. Characteristics of the cats.
| Parameters (Mean ± SEM) | Total (n = 28) | Group 1 (n = 17) | Group 2 (n = 6) | Group 3 (n = 5) | p-value |
|---|---|---|---|---|---|
| Age (years) | 5.34 ± 2.25 | 5.32 ± 2.67 | 5.83 ± 0.69 | 4.80 ± 1.72 | 0.7711 |
| Weight (kg) | 3.50 ± 0.85 | 3.57 ± 1.01 | 3.20 ± 0.52 | 3.60 ± 0.28 | 0.6515 |
| Male, n (%) | 50 | 47 | 50 | 60 | – |
| Cyst in both kidneys, n (%) | 39.28 | 0 | 100 | 100 | – |
SEM = Standard error of the mean, n = Number of cats, – = Not applicable (no statistical comparison performed for categorical variables in this context).
Ultrasonographic findings
Renal ultrasonographic findings for all cats are presented in Table 2. Cats in Groups 2 and 3 exhibited multiple, well-defined anechoic renal cysts with distal acoustic enhancement, consistent with polycystic kidney morphology. Cysts were bilaterally distributed in affected cats and varied in size and number. Significant differences in kidney length and height were observed among groups, reflecting structural renal remodeling in cats with cystic disease. In contrast, the kidney-to-aortic diameter ratio did not differ significantly among groups, indicating consistent normalization for body size across populations. Representative ultrasonographic images are shown in Figure 1.
Table 2. Ultrasonographic parameters.
| Parameters (Mean ± SD) | Total (n = 28) | Group 1 (n = 17) | Group 2 (n = 6) | Group 3 (n = 5) | p-value |
|---|---|---|---|---|---|
| Average kidney length (cm) | 4.04 ± 0.86 | 3.76 ± 0.45 | 4.07 ± 0.59 | 4.93 ± 1.39 | 0.0001 |
| Average kidney length/aorta | 13.90 ± 2.42 | 13.89 ± 2.28 | 14.51 ± 2.12 | 13.85 ± 2.98 | 0.7977 |
| Average kidney height (cm) | 2.18 ± 0.48 | 2.02 ± 0.29 | 2.06 ± 0.27 | 3.01 ± 0.49 | 0.0271 |
| Systolic blood pressure (mmHg) | 137.64 ± 18.69 | 139.09 ± 16.62 | 141.72 ± 20.39 | 128.40 ± 19.92 | 0.4820 |
SD = Standard deviation, n = Number of cats,
* p < 0.05,
**p < 0.01,
*** p < 0.0001. A statistically significant difference was observed among groups using analysis of variance.
Hematological and biochemical profiles
Hematological and biochemical parameters for all cats (n = 28) are summarized in Table 3. To minimize confounding effects, cats with pre-existing hematologic disorders, diagnosed chronic kidney disease, or a history of anticoagulant therapy were excluded before analysis. Mean concentrations of creatinine, blood urea nitrogen, and SDMA did not differ significantly among groups (p > 0.05), indicating preserved renal excretory function across all study populations. Similarly, total plasma protein and CRP concentrations showed no statistically significant intergroup differences.
Table 3. Blood profiles of all cats.
| Parameters (Mean ± SD) | Total (n = 28) | Group 1 (n = 17) | Group 2 (n = 6) | Group 3 (n = 5) | p-value |
|---|---|---|---|---|---|
| Plasma Cr concentration (mg/dL) | 1.26 ± 0.32 | 1.26 ± 0.27 | 1.46 ± 0.38 | 1.10 ± 0.32 | 0.1939 |
| BUN (mg/dL) | 21.33 ± 3.59 | 20.94 ± 3.59 | 21.13 ± 2.82 | 22.88 ± 1.78 | 0.5905 |
| SDMA (μg/dL) | 16.67 ± 2.11 | 17.21 ± 1.65 | 16.0 ± 1.29 | 15.20 ± 3.12 | 0.1458 |
| TP (g/dL) | 7.27 ± 0.49 | 7.19 ± 0.50 | 7.21 ± 0.39 | 7.63 ± 0.37 | 0.2025 |
| NLR | 4.68 ± 4.0 | 3.82 ± 1.77 | 9.17 ± 8.13 | 4.09 ± 1.80 | 0.0508 |
| MLR | 0.17 ± 0.11 | 0.17 ± 0.11 | 0.11 ± 0.05 | 0.28 ± 0.13 | 0.0534 |
| PLR | 166.14 ± 27.00 | 147.07 ± 17.00 | 155.97 ± 6.00 | 258.19 ± 4.00 | 0.3031 |
| CRP (mg/dL) | 0.13 ± 0.05 | 0.15 ± 0.05 | 0.12 ± 0.04 | 0.10 ± 0.01 | 0.0843 |
SD = Standard deviation, n = Number of cats, Cr = Creatinine, BUN = Blood urea nitrogen, SDMA = Symmetric dimethylarginine, TP = Total plasma protein, NLR = Neutrophil-to-lymphocyte ratio, MLR = Monocyte-to-lymphocyte ratio, PLR = Platelet-to-lymphocyte ratio, CRP = C-reactive protein,
* p < 0.05,
**p < 0.01, ***p < 0.0001. A statistically significant difference was observed among groups using analysis of variance.
In contrast, inflammatory cell ratios demonstrated notable trends. NLR tended to be higher in Group 2 (9.17 ± 8.13) compared with Group 1 (3.82 ± 1.77) and Group 3 (4.09 ± 1.80), approaching statistical significance (p = 0.0508). MLR showed a similar borderline difference (p = 0.0534), with higher values observed in Group 3 (0.28 ± 0.13). PLR was numerically elevated in Group 3 (258.19 ± 4.00), although this difference did not reach statistical significance.
Correlation between inflammatory biomarkers and ultrasonographic parameters
Correlation matrixes are illustrated in Figures 2 and 3. In clinically healthy cats (Group 1), moderate positive correlations were observed among inflammatory ratios, particularly between NLR and PLR (r = 0.86) and between NLR and MLR (r = 0.62). However, inflammatory biomarkers showed weak or negligible associations with renal biochemical indices and kidney morphometric measurements. In contrast, cats with renal cysts (Groups 2 and 3 combined) demonstrated markedly stronger correlations. NLR correlated strongly with PLR (r = 0.94) and showed positive associations with blood urea nitrogen (r = 0.71), creatinine (r = 0.63), SDMA (r = 0.62), and kidney morphometrics (length r = 0.82, height r = 0.75). PLR also correlated positively with blood urea nitrogen (r = 0.81) and creatinine (r = 0.61). These findings indicate an emerging link between low-grade systemic inflammation and structural renal changes in cats with cystic kidney disease, even in the absence of overt renal dysfunction.
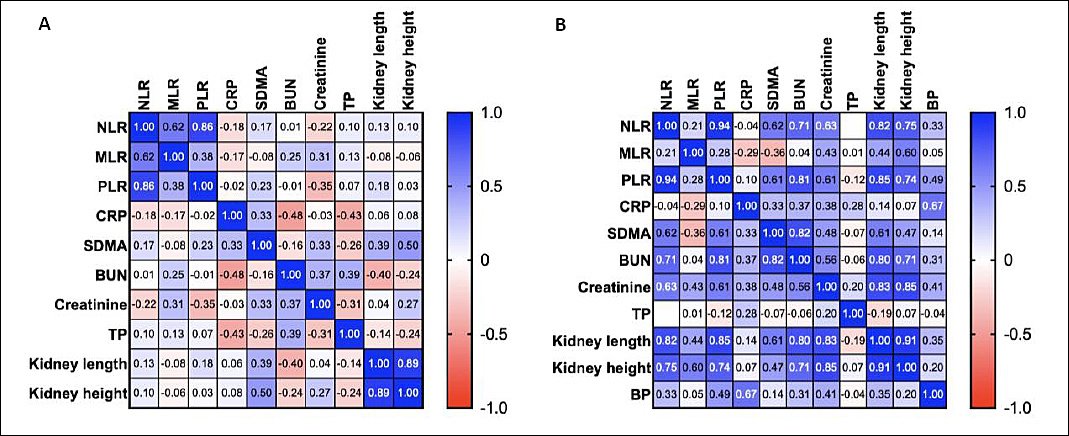
Figure 2. Heatmap of the Pearson correlation matrix showing relationships among hematological inflammatory ratios (NLR, MLR, and PLR), biochemical markers (CRP, SDMA, BUN, creatinine, and TP), and renal morphometric parameters (kidney length, kidney height). (A) Cats without renal cysts. (B) Cats with renal cysts.
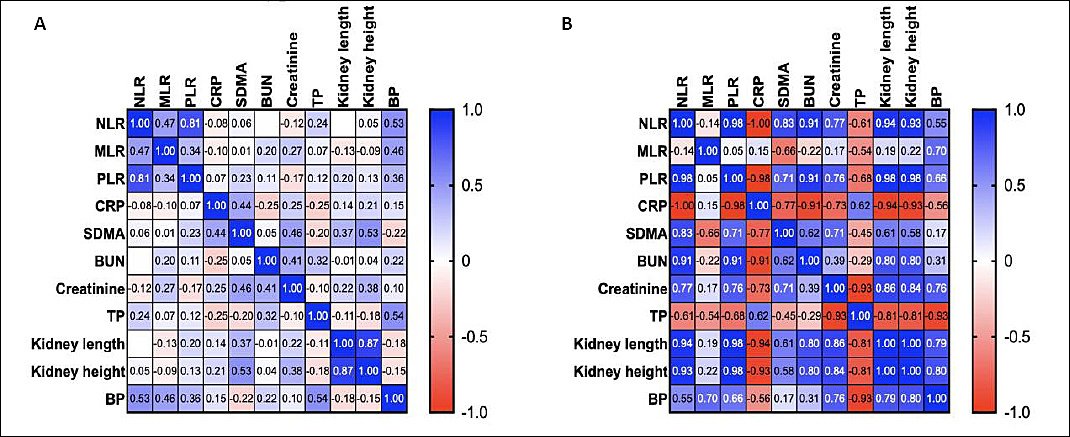
Figure 3. Correlation matrix of hematological inflammatory ratios (NLR, MLR, and PLR), biochemical markers (CRP, SDMA, BUN, creatinine, and TP), and
Pathological and molecular considerations
No gross pathological specimens, histopathological slides, or postmortem findings were available, as all cats were alive, clinically stable, and managed under standard clinical care. Consequently, renal histopathology and downstream molecular pathway analyses were beyond the scope of this retrospective study. Molecular investigation was limited to
DISCUSSION
Overview of principal findings
This study examined the relationship between systemic inflammatory indices, renal structure, renal function, and
Inflammatory indices in early and subclinical PKD
Previous studies on feline PKD have focused largely on genetic diagnosis and imaging characteristics, with limited emphasis on systemic inflammatory responses during early disease stages. Consistent with earlier reports, cats in the present study showed normal creatinine, blood urea nitrogen, and SDMA concentrations, indicating preserved renal excretory function in early or compensated PKD [15, 16]. Similar observations have been reported in both feline and human PKD, where substantial nephron loss may occur before biochemical markers exceed reference ranges.
Despite stable renal biomarkers, NLR, MLR, and PLR demonstrated distinct group-related trends, suggesting early immune activation. The elevated NLR observed in cats with cystic kidneys and wild-type
In contrast, the higher MLR observed in cats carrying a
CRP and platelet-related responses
CRP concentrations did not differ significantly among groups, in agreement with previous feline studies reporting limited sensitivity of CRP in chronic, low-grade inflammatory conditions, particularly renal disease. Unlike acute inflammatory disorders, PKD progression is insidious, and systemic CRP responses may remain subdued until advanced stages.
The numerical increase in PLR observed in cats with
Relationship between inflammation, renal structure, and function
Correlation analyses demonstrated a progression from weak associations in healthy cats to strong, multivariate correlations in cats with cystic kidneys and
These findings parallel observations in human PKD, where kidney enlargement correlates more closely with disease progression than early biochemical markers [20, 21]. The strong associations between inflammatory indices and renal morphometrics in
Genetic influence and molecular pathophysiology
The amplified correlations observed in cats carrying
The observed relationships between inflammatory markers, renal function indices, and blood pressure in
Clinical implications
The results suggest that hematological inflammatory ratios, particularly NLR and MLR, may serve as accessible and cost-effective tools for identifying early inflammatory activity in cats with renal cysts, even before the development of azotemia. Integration of these indices with ultrasonography and genetic testing may enhance risk stratification, disease monitoring, and early intervention strategies in feline PKD.
Limitations
This study has several limitations. The sample size was relatively small, which may limit statistical power and generalizability. As a retrospective, single-center study, environmental influences, dietary factors, and subclinical comorbidities could not be fully controlled. Because all cats were alive and clinically stable, histopathological confirmation and postmortem evaluation were not available, precluding direct assessment of renal fibrosis, inflammatory infiltrates, and cyst wall pathology. Molecular analyses were limited to
CONCLUSION
This study demonstrated that systemic inflammatory activation is detectable in cats with renal cystic disease despite preserved conventional renal biomarkers, including creatinine, blood urea nitrogen, and SDMA. Inflammatory indices derived from routine hematology, particularly NLR and MLR, showed stronger associations with renal morphometric parameters and biochemical indices in cats with renal cysts than in clinically healthy controls. These associations were most pronounced in cats carrying a heterozygous
The findings suggest that simple hematological inflammatory ratios, such as NLR and MLR, may serve as accessible, low-cost adjunct tools for early detection and monitoring of PKD in cats. When used alongside ultrasonography and
A key strength of this study is the integrated evaluation of systemic inflammation, renal morphometrics, biochemical markers, and
Future studies should incorporate larger, multicenter cohorts with longitudinal follow-up to validate the prognostic value of inflammatory ratios in PKD. Integration of repeated inflammatory assessments, advanced imaging modalities, and histopathological and molecular analyses will be essential to clarify the temporal relationship between inflammation, cyst expansion, and renal dysfunction. Evaluating the response of inflammatory indices to therapeutic interventions may also provide insight into their utility as monitoring biomarkers.
Overall, this study supports the concept that systemic inflammation is an early and integral component of feline PKD, particularly in cats carrying
DATA AVAILABILITY
All the generated data are included in the manuscript.
AUTHORS’ CONTRIBUTIONS
SP: Identified the research topic and study area and drafted the manuscript. SP and KJ: Performed the study, developed the methodology, and conducted data analysis and interpretation. KJ, PJ, WM, and RB: Analyzed and interpreted the data and revised the manuscript. All authors have read, reviewed, and approved the final version of the manuscript.
COMPETING INTERESTS
The authors declare that they have no competing interests.
ACKNOWLEDGMENTS
The authors would like to thank the Faculty of Veterinary Medicine, Kasetsart University, and Kasetsart University Veterinary Teaching Hospital, Kamphaengsaen, for granting permission to conduct this study. The authors gratefully acknowledge the partial financial support provided by the Faculty of Veterinary Medicine, Kasetsart University Research Fund under a Research Scholar contract (66/11) awarded to Kotchapol Jaturanratsamee.
REFERENCES
- Lyons LA. DNA mutations of the cat:the good, the bad, and the ugly. J Feline Med Surg 2015;17(3):203-219. [Google Scholar] | [Crossref]
- Barrs VR, Gunew M, Foster SF, Beatty JA, Malik R. Prevalence of autosomal dominant polycystic kidney disease in Persian and related breeds in Sydney and Brisbane. Aust Vet J 2001;79(4):257-259. [Google Scholar] | [Crossref]
- Bonazzi M, Volta A, Gnudi G, Bottarelli E, Gazzola M, Bertoni G. Prevalence of polycystic kidney disease and renal and urinary bladder ultrasonographic abnormalities in Persian and Exotic Shorthair cats in Italy. J Feline Med Surg 2007;9:387-391. [Google Scholar] | [Crossref]
- Ghys LF, Meyer E, Paepe D, Delanghe J, Daminet S, Lefebvre HP. Evaluation of symmetric dimethylarginine in cats with kidney disease. J Vet Intern Med;2016(30):173-181. [Google Scholar] | [Crossref]
- Schirrer L, Marín-García PJ, Llobat L. Feline polycystic kidney disease:an update. Vet Sci 2021;8(11):269. [Google Scholar] | [Crossref]
- Montllor L, Mañú-Pereira MD, Llaudet-Planas E, Gómez Ramírez P, Sevilla Navarro J, Vives-Corrons JL. Red cell pyruvate kinase deficiency in Spain:a study of 15 cases. Med Clin (Barc) 2017;148(1):23-27. [Google Scholar] | [Crossref]
- Lyons LA, Biller DS, Erdman CA, Lipinski MJ, Young AE, Roe BA. Feline polycystic kidney disease mutation identified in
PKD1 . J Am Soc Nephrol 2004;15:2548-2555. [Google Scholar] | [Crossref] - Domanjko-Petrič A, Černec D, Cotman M. Polycystic kidney disease:a review and occurrence in Slovenia with comparison between ultrasound and genetic testing. J Feline Med Surg 2008;10(2):115-119. [Google Scholar] | [Crossref]
- Jaturanratsamee K, Jiwaganont P, Sukumolanan P, Petchdee S.
PKD1 gene mutation and ultrasonographic characterization in cats with renal cysts. F1000Res 2024;12:760. [Google Scholar] | [Crossref] - Boag AK, Letendre JA, Gillis TE, Harkin KR, Polzin DJ, Cowgill LD. Association of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio with inflammation and outcome in canine kidney disease. J Vet Intern Med;2018(32):1853-1861. [Google Scholar] | [Crossref]
- Jiwaganont P, Jaturanratsamee K, Thaisakun S, Roytrakul S, Petchdee S. Analysis of serum proteomics in cats with polycystic kidney disease-1 gene mutation. Heliyon 2024;10(15):e35577. [Google Scholar] | [Crossref]
- Hall JA, Yerramilli M, Obare E. Relationship between symmetric dimethylarginine and glomerular filtration rate in cats with chronic kidney disease. J Vet Intern Med;2014(28):1676-1683. [Google Scholar] | [Crossref]
- Nabity MB, Hokamp JA. Urinary biomarkers of kidney disease in dogs and cats. Vet Clin North Am Small Anim Pract 2023;53(1):53-71. [Google Scholar] | [Crossref]
- Jaturanratsamee K, Choisunirachon N, Soontornvipart K, Darawiroj D, Srisowanna N, Thanaboonnipat C. Ultrasonographic kidney length-to-abdominal aortic diameter for diagnosis of feline chronic kidney disease. Vet World 2023;16(5):1114-1121. [Google Scholar] | [Crossref]
- Paltrinieri S, Giordano A, Stranieri A, Lauzi S, Ceciliani F. C-reactive protein in cats:diagnostic and prognostic relevance in inflammation and renal disease. Vet J 2021;274:105726. [Google Scholar] | [Crossref]
- Ceribasi AO, Ceylan A, Ozkan C, Ocal N, Aksoy O. Evaluation of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as biomarkers in cats with chronic kidney disease. J Feline Med Surg 2020;22(9):855-862. [Google Scholar] | [Crossref]
- Syme HM, Markwell PJ, Pfeiffer D, Elliott J. Structural and functional correlations in feline polycystic kidney disease. Vet J 2017;228:1-8. [Google Scholar] | [Crossref]
- Torres VE, Chapman AB, Devuyst O, Gansevoort RT, Grantham JJ, Higashihara E. Inflammation and fibrosis in polycystic kidney disease:emerging therapeutic targets. Nat Rev Nephrol 2020;16(3):137-150. [Google Scholar] | [Crossref]
- Zhang X, Wang X, Wang T, Lin Q, Fang Z, Zhang Y. Role of inflammatory signaling in the progression of autosomal dominant polycystic kidney disease. Kidney Int 2020;98(6):1379-1393. [Google Scholar] | [Crossref]
- Buturović-Ponikvar J, Višnar-Perovič A. Ultrasonography in chronic renal failure. Eur J Radiol 2003;46(2):115-122. [Google Scholar] | [Crossref]
- Debruyn K, Haers H, Combes A, Paepe D, Peremans K, Saunders JH. Ultrasonography of the feline kidney:technique, anatomy, and changes associated with disease. J Feline Med Surg 2012;14(11):794-803. [Google Scholar] | [Crossref]
- Chew DJ, DiBartola SP, Schenck PA, Grauer GF, Lees GE, Forrester SD. Pathophysiology and management of feline polycystic kidney disease. Vet Clin North Am Small Anim Pract 2022;52(1):71-87. [Google Scholar] | [Crossref]
- Leierer J, Kerschbaum J, Mayer G, Rudnicki M, Heerspink HJL, Scherberich JE. Coregulation analysis of mechanistic biomarkers in autosomal dominant polycystic kidney disease. Int J Mol Sci 2021;22(13):6885. [Google Scholar] | [Crossref]
- Jovanović D, Gašić B, Pavlović S, Naumović R. Correlation of kidney size with kidney function and anthropometric parameters in healthy subjects and patients with chronic kidney disease. Ren Fail 2013;35(6):896-900. [Google Scholar] | [Crossref]